Skip to content
thebodyjunction@gmail.com
Pilates Only : 01424 215300
Therapists
Book A Class
Online Video Classes
The Body Junction | Pilates, Yoga & Therapies in Bexhill
Pilates, Yoga, Therapy, Physiotherapy
Home
What We Offer/Timetable
Pilates
Summer Timetable
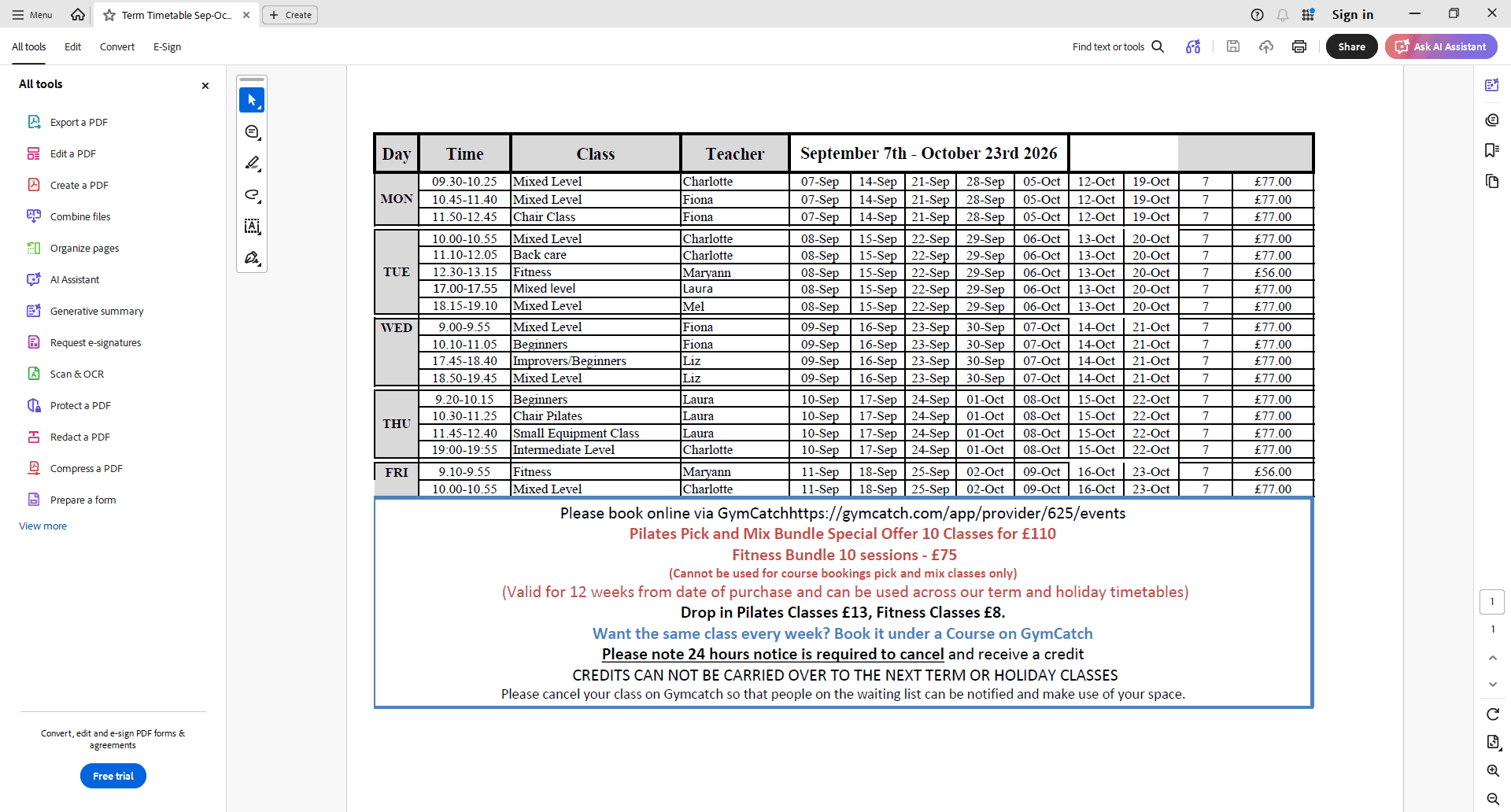
September-October Timetable
Book a Class
Pilates what we offer
GymCatch User Guide
New Client Questionnaire
Yoga
Pricelist & Therapist Details
The Body Junction Price List
Book a Pilates Class
About Us
Pilates Team
Therapists
Physiotherapists
Blog
Videos
Testimonials
Contact Us
Newsletter & Sign Up
Newsletter
Subscribe to Newsletter
Gift Vouchers
Home
What We Offer/Timetable
Pilates
Summer Timetable
September-October Timetable
Book a Class
Pilates what we offer
GymCatch User Guide
New Client Questionnaire
Yoga
Pricelist & Therapist Details
The Body Junction Price List
Book a Pilates Class
About Us
Pilates Team
Therapists
Physiotherapists
Blog
Videos
Testimonials
Contact Us
Newsletter & Sign Up
Newsletter
Subscribe to Newsletter
Gift Vouchers
Questionnaire
Please enable JavaScript in your browser to complete this form.
Full Name
*
First
Last
Email
*
Date Of Birth (dd/mm/yyyy)
Occupation
Address + PostCode
Phone Number
*
Subscribe To Our Mailing List?
*
Yes
No
We occasionally send emails/newsletters relating to the classes and therapies we provide here. Do you wish for us to add your email to our mailing list? You can unsubscribe to this at any time by scrolling to the bottom of one of our newsletters and clicking 'Unsubscribe' within the email.
Doctor
Have You Done Pilates Before?
Yes
No
If yes, who with and how long for?
Do you do any of these?
Yoga
Aerobics
Do You Exercise? If so, what exercise do you do?
Have you had children. If yes, how many? Did you have a difficult birth? Can you engage your pelvic floor muscles?
Do you have an injury or current area of pain i.e. Back or Neck pain? (if yes, please specify where)
Have you had major surgery with the last year? If yes, when and what surgery was for?
Are you currently receiving treatment from a chiropractor, osteopath or physiotherapist? If yes, who?
Are you currently on any medication, or seeing a specialist for any reason?
Do you have high or low blood pressure?
Yes
No
Do you suffer with aches and pains in your bones or joints?
Yes
No
Are there any movements you know you can or should not do? (i.e. kneeling)
Are you able to lie on both sides?
Yes
No
Are you able to get up and down from the floor?
Yes
No
Can you lie on your back and your front?
Yes
No
How would you describe your health?
Do You Do Any Of The Following?
Sit with your feet up
Read in bed/watch TV in bed
Have long soaks in the bath
Sit on sofa with feet to one side
Cross your legs
Have your TV/computer screen to one side
Sleep on your tummy
Use a laptop
Where Did You Hear About Us?
What Do You Hope To Achieve From Doing Pilates?
What classes are you interested in joining?
*
Induction/Beginner Classes
Mixed Level Pilates
Other Classes
Client Release Statement. I willingly participate in the practical exercises at my own risk. Despite any possible restrictions , disabilities or any predisposition to sickness or injury that may be aggravated or adversely affected as a result of my participation, I take full responsibility for any injury, loss or damage to my person or property that may arise directly or indirectly from my participation in the exercises. I will not seek to penalize, prosecute or claim compensation from the company for any injury, loss or damage. Signed:
*
Date Signed
*
Submit Questionnaire
Go to Top
{kind=link}